 |
| Dietary protein sources: You better eat them before they're rancid. |
There's such a thing as "protein oxidation"? If you are asking yourself this question, you will probably have missed the 20th century studies by Henry D. Dakin (*1880–†1952). Dakin originally reported the oxidative degradation of particular amino acids during digestion and introduced the potential biological consequences of such biochemical reactions.
The impact of PROTOX, as this form oxidation is called to distinguish it from the way better known LOX (lipid oxidation) on human health was, at that moment, wholly unknown.
As Estévez and Luna point out in a recent paper in the peer-reviewed scientific journal "Critical Reviews in Food Science and Nutrition", PROTOX has been in the focus during the succeeding decades, though, "owing to the association between the oxidative damage to proteins and aging and age-related diseases (Berlett & Stadtman, 1997)" (Estévez. 2016).
Learn more about meat at the SuppVersity 
You May Eat Pork, too!

You Eat What You Feed!

Meat & Prostate Cancer?

Meat - Is cooking the problem

Meat Packaging = Problem?

Grass-Fed Pork? Is it Worth it?
Earl R. Stadtman (*1919–†2008), a renowned biochemist of the 20th century and mentor of various Novel-prized scientists, was one of the pioneers in unveiling the chemistry and biological consequences of PROTOX. From the elucidation of mechanisms whereby the rates of metabolic reactions match to the necessities of the living cell, he identified the connection between unbalanced oxidative metabolism (≈ oxidative stress) and impaired physiological processes (Stadtman, 1990).
 |
| Figure 1: Oxidative damage to poultry: Sources of oxidative stress, impact of oxidation, and antioxidant strategies (Estévez. 2015). |
"While some of the underlying mechanisms of the connection between in vivo PROTOX and disease are still to be clarified, it is accepted that PROTOX plays a role in aging and age related diseases such as Alzheimer’s, Parkinson’s, inflammatory Bowel’s (IBD), rheumatoid arthritis, diabetes, muscular dystrophy, and cataractogenesis, among others (Berlett & Stadtman, 1997).
On account of the effort of brilliant scientists, the ‘poor cousin’ of lipid oxidation is now extolled as a topic of the utmost scientific interest" (Estévez. 2016).
Now that you know all that, I suspect that you are asking yourself what this "protein oxidation" has to do with "Food Science and Nutrition". Well, the answer is actually pretty simple: While PROTOX has been for decades disregarded as a major cause of food deterioration, it does play a major role in foods from nutritional, sensory and technological points of view.
Note: There will be a follow up to this article, next week with answers to your questions, such as (1) How can I avoid protein oxidation when preparing protein containing meals? (2) Which foods are the most susceptible? (3) If processing is an issue won't protein powders be the worst offenders? Not your question? Feel free to post additional questions you may have
here.
In the early years of the 21st century, numerous subsequent studies shed light on the oxidative modifications undergone by muscle proteins during handling, processing and storage of muscle foods; and among of the better known results of these studies are...
 |
| Figure 2: Hypothesis of the influence of dietary protein oxidation on in vivo oxidative stress and pathological conditions. "It is actually well-established that the composition of food and the dietary habits have physiopathological consequences" (Estévez. 2016). |
- that the formation of PROTOX will impair the functionality and digestibility of meat and dairy proteins (Santé-Lhoutellier et al., 2007; Feng et al., 2015),
- that the presence of PROTOX will impair the nutritional value and sensory attributes of muscle foods such as tenderness (Bao & Ertbjerg, 2015) and flavor (Villaverde et al., 2014), and the chemistry behind food PROTOX, the occurrence and consequences of PROTOX during food
- that PROTOX will almost inevitably occur during storage and processing, but can be reduced by applying certain strategies (Bekhit et al., 2013; Estévez, 2015; Soladoye et al., 2015).
As Estévez and Luna point out, the investigation of postprandial events, which has started, only recently, "enables a more realistic approach to investigate the impact of food intake on nutrition and health as food components are severely modified during the digestion phases" (Estévez. 2016). Unfortunately, many of the currently existing studies investigated events in-vitro. The important (and certainly most relevant) question, whether the consumption of oxidized proteins from food can actually harm you, however, has been addressed by a limited number of studies, only.
How to prevent protein oxidation? There's no way you prevent the oxidation of proteins in food completely, but packaging in light-blocking low-oxygen containers and not processing foods like crazy (exerting force on it in a grinder, for example | see
Figure, right. Bao. 2015) could reduce the oxidation process just as significantly as not heating / burning meat will (Villaverde. 2013).
There's, nevertheless, "evidence that in vivo oxidation is a source of aging and disease calls to elucidate to which extent dietary oxidative stress contributes to aggravating in vivo oxidative stress and its harmful consequences" (Estéves. 2015); and these "harmful consequences" have been traced back to particular dietary oxidation products, of which researchers believe that they are able to induce or contribute to some pathological process in targeted cells or tissues through the induction of specific molecular responses (i.e. gene expression regulation).
 |
| Figure 2: Proposed mechanisms of pathogenesis exerted by dietary protein oxidation products. It was not until recently that the fact that dietary oxidized proteins would, themselves, be active executors of specific pathological processes was discovered (Estévez. 2016). |
the intake of foods high in PROTOX products, raises general oxidation markers, leads to cell damage and increases the risk of suffering health disorders such as coronary-heart diseases, neurodegenerative disorders and certain types of cancer (Esterbauer et al., 1992, 1993; Sies et al., 2005; Awada et al., 2012), - interestingly, these processes have been linked to LOX products, as well, which turn out to be cross-linked to the cytotoxicity and mutagenicity potential of PROTOX species on the gastrointestinal tract or in internal organs upon absorption (Esterbauer et al., 1993),
- proteins are regarded as targets for post-translational changes, unlike LOX of which we believe that they have a direct damaging effect
- the molecular basis of these processes commonly involves the interaction of primary and secondary LOX products (i.e. alkyl radicals, peroxides, hexanal, 4-HNE, MDA) with proteins of biological significance (formation of adducts) and other biomolecules such as DNA (Esterbauer et al., 1991; Awada et al., 2012).
- cellular responses to these molecular changes usually imply the activation of particular signalling pathways that involves gene expression and/or suppression (Figure 2),
Now, while all of this has been known for years, it was not until recently that the fact that dietary oxidized proteins and PROTOX products would, themselves, be active executors of specific pathological processes was discovered.
"The oxidation of food proteins during processing and storage leads to the inexorable accumulation of oxidation products that will be primary exposed to the gastrointestinal tract. As aforementioned, food PROTOX also occurs during consumption and gastrointestinal digestion increasing the concentration of oxidation products in the lumen. Scientific evidences support the impact of dietary oxidized proteins on intestinal flora disturbance, the redox state of intestinal tissues and the onset of local pathological conditions (Keshavarzian et al., 2003; Fang et al., 2012; Xie et al., 2014).
Pierre et al. (2004), among others, already provided reasonable arguments to support the impact of luminal oxidative stress on cytotoxicity, genotoxicity and apoptosis in cells from colonic mucosa. More specifically, oxidative stress has been found to play a relevant role in the onset of carcinogenic processes, including CRC (Polyak et al., 1997; Valko et al., 2006). Interestingly, some clinical studies emphasize the extent of plasma protein carbonylation as a reliable marker of the risk of suffering CRC (Yeh et al., 2010; Chang et al., 2008). Chang et al. (2008) in particular, found altered protein carbonyl levels in CRC patients while LOX products remained at low levels. Others implicate the oxidative damage to proteins in the pathogenesis of CRC. This is the case of Nedic et al. (2013) who indicated the potential role of the carbonylation of insulin-like growth factor-binding proteins in CRC growth" (Estévez. 2016).
While the formerly cited evidence is mostly from in vitro studies, more recent data from rodents shows that intraperitoneal administration (= injection that is equivalent to oral consumption) of oxidized proteins to rats raised the level of advanced oxidation protein products )AOPPs) in the local intestine tissue
and in blood inducing intestine epithelial death through a redox-dependent
pathway. As Estévez and Luna rightly point out, "[t]hese results proven that PROTOX products may be implicated in the transfer of oxidative stress from the luminal phase to the lamina propia of the intestinal mucosa facilitating the process of IBD" (Estézes. 2016 |see Figure 4, left).
 |
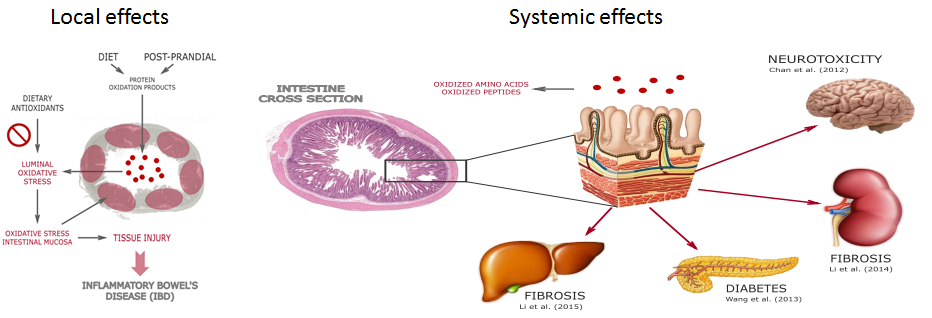
| Figure 4: LEFT - Pathogenesis of dietary protein oxidation products in the GIT: transfer of oxidative stress from lumen to intestinal mucosa, tissue injury and inflammatory disease.f, RIGHT - Absorption and subsequent pathological effects of dietary protein oxidation products in targeted tissues (Estévez. 2016). |
The molecular mechanisms of this pathological effect involved is, according to the authors of this most recent review a NADPH oxidase-mediated ROS generation, JNK phosphorylation, and poly (ADP-ribose) polymerase-1 (PARP-1) activation. Consequences of which studies show that their effects are not limited to the gut.
 |
| Protein oxidation during refrigerated storage of liver pâtés with added BHT sage or rosemary essential oils (p < 0.05, between antioxidant groups within a day of storage denoted by letters | Estévez. 2006) |
Vitamin E doesn't work, vitamin C only increases the formation of PROTOX! Studies suggest that adding known anti-oxidant to your foods may both promote and inhibit the formation of PROTOX or Pox, as they are also called. The usual suspects, such as tocopherols, however, will be failing you, here. Some phenolic-rich plant and fruit extracts have been shown to exert anti-oxidative protection of proteins in cooked pork patties, porcine liver pâté (see figure on the left) and chicken, but the pro-/anti-oxidative effect depends on the structure and the concentration of the respective phenolic compound.
In beef patties, a rosemary extract was found to have no protective effect against Pox and a mixture of ascorbate and citrate promoted Pox, while both anti-oxidant systems protected lipids from oxidation. Furthermore, addition of rosemary oil to frankfurters has been shown to inhibit Pox while addition of higher levels of the rosemary oil resulted in a prooxidative effect when the frankfurters were prepared with meat from white pigs showing that the anti-oxidative effect was dependent on concentration and product characteristics. Lastly, it should be mentioned that the synthetic hydrophilic anti-oxidant Trolox (a vitamin E analogue) was found to prevent oxidation of both protein and lipid fractions (Lund. 2011).
As such, diets rich in readily oxidized components (polyunsaturared fatty acids) and meat proteins are believed have long been linked to a increased risk of suffering various forms of IBD such as Crohn's disease and ulcerative colitis (Hou et al., 2011), but it is also, as Estévez and Luna point out, also reasonable to hypothesize that such diets may contribute considerable oxidized proteins given the close association between LOX and PROTOX in food systems and in the gastrointestinal tract (Soladoye et al., 2015; Van-Hecke et al., 2015).
"Gurer-Orhan et al. (2006) already hypothesized that oxidized amino acids may be misincorporated into proteins such as enzymes and structural element in cells, potentially contributing to malfunction, cell apoptosis and disease. These authors emphasized that post-translational oxidative modification of proteins may not be the only factor that contributes to in vivo PROTOX suggesting that external (dietary) sources of oxidized amino acids may cause direct toxic effects by being used for de novo synthesis of proteins. To similar conclusions came succeeding studies carried out by Dunlop et al. (2008; 2011). The absorption and subsequent deleterious effects of unnatural oxidized amino acids such as meta-tyrosine and 3,4-dihydroxyphenylalanine (L-DOPA) are known to occur in animals and humans leading to dysfunctional proteins and toxicity (Dunlop et al., 2015). These species may not only be formed in foods as a result of tyrosine oxidation, they are also natural components of edible plants and beans (Siddhuraju & Becker, 2001; Davies, 2003; Dunlop et al., 2015). Chan et al. (2012) demonstrated that substitution of L-tyrosine residues in proteins with L-DOPA causes protein misfolding, promotes protein aggregation and stimulates the formation of autophagic vacuoles in SH-SY5Y neuroblastoma cells. Other oxidized forms of tyrosine, such as the ortho-tyrosine, contribute to the impairment of the insulin-induced arterial relaxation through the attenuation of endothelial nitric oxide synthase (eNOS) phosphorylation (Szijártó et al., 2014)" (Estévez. 2016).
Similar effects as they are described for oxidized tyrosine have been observed for oxidized tryptophan and lysine, which are present in significant amount in a plethora of processed foods including, but not restricted to meat and dairy.
 |
| Table 1: Relation of 2-AAA (oxidized lysine) levels to the risk of future diabetes in the whole sample and subgroups of 188 individuals who developed diabetes and 188 propensity-matched controls from 2,422 normoglycemic participants followed for 12 years in the Framingham Heart Study (Wang. 2013). |
With respect to the latter, i.e. oxidized lysine, it is certainly worth poining out that 12-years long metabolomic study with human patients found this compound to be the most reliable indicator of diabetes risk - plus: Wang et al. were able to demonstrate that its oral ingestion increased the levels of the oxidized amino acid particularly in the pancreas, the same organ that is failing in diabetes (Wang et al., 2013). Other oxidized amino acids have been linked to
- cell death in the intestine, colon and small intestine and subsequent irritable bowel disease (various) AOPPs; Xie et al (2014), Fang et al. (2012), Keshavarzian et al. (2003), Wu et al. (2015)
- intestinal flora & redox state disturbance and liver & kidney stress, oxidized casein; Fang et al. (2012), Li et al. (2013), and Li et al. (2014)
With oxidized proteins and amino acids, there's thus yet another, often overlooked parameter of our food intake and dietary habits with "straightforward impact on health status" (Estevéz. 2016).
Bottom line: As premature as our understanding of the biology that governs the beneficial/detrimental effects of certain dietary components still is, there is ample evidence that not just the consumption of oxidized dietary fats, but also that of proteins, the major components of most foods (particularly animal-source), could harm us.
 |
| Fresh (!) Red Meat Acquitted - Overgeneralized Accusations that Red Meat Consumption Triggers Cancer Overlooks Influence of Processing & Other Confounding Factors | more |
This does not mean that proteins (animal or plant proteins) are still a vital part of a healthy diet - that's indisputable. As Estevez and Luna point, out, "the discussion about dietary proteins [wich] is typically centered in the quantity, quality (≈ amino acid profile; biological value) and bioavailability upon digestibility," future recommendations for protein intake will have to consider the differential impact of foods with different PROTOX levels, as well. In this context, it should be obvious why "the current increase of the intake by population of highly processed animal-based foods with high protein content and presumably high oxidation rates" has been found to predict the raise of health disorders already associated to in vivo or dietary oxidative stress, in dozens if not hundreds of epidemiological studies |
Comment!
References:
- Awada, Manar, et al. "Dietary oxidized n-3 PUFA induce oxidative stress and inflammation: role of intestinal absorption of 4-HHE and reactivity in intestinal cells." Journal of lipid research 53.10 (2012): 2069-2080.
- Bao, Yulong, and Per Ertbjerg. "Relationship between oxygen concentration, shear force and protein oxidation in modified atmosphere packaged pork." Meat science 110 (2015): 174-179.
- Berlett, Barbara S., and Earl R. Stadtman. "Protein oxidation in aging, disease, and oxidative stress." Journal of Biological Chemistry 272.33 (1997): 20313-20316.
- Chan, Sandra W., et al. "L-DOPA is incorporated into brain proteins of patients treated for Parkinson's disease, inducing toxicity in human neuroblastoma cells in vitro." Experimental neurology 238.1 (2012): 29-37.
- Chang, Dong, et al. "Evaluation of oxidative stress in colorectal cancer patients." Biomedical and Environmental Sciences 21.4 (2008): 286-289.
- Davies, Michael J. "Singlet oxygen-mediated damage to proteins and its consequences." Biochemical and biophysical research communications 305.3 (2003): 761-770.
- Davies, Michael J. "The oxidative environment and protein damage." Biochimica et Biophysica Acta (BBA)-Proteins and Proteomics 1703.2 (2005): 93-109.
- Dunlop, Rachael A., Roger T. Dean, and Kenneth J. Rodgers. "The impact of specific oxidized amino acids on protein turnover in J774 cells." Biochemical Journal 410.1 (2008): 131-140.
- Dunlop, Rachael A., Ulf T. Brunk, and Kenneth J. Rodgers. "Proteins containing oxidized amino acids induce apoptosis in human monocytes." Biochemical Journal 435.1 (2011): 207-216.
- Estévez, Mario, Sonia Ventanas, and Ramón Cava. "Effect of natural and synthetic antioxidants on protein oxidation and colour and texture changes in refrigerated stored porcine liver pâté." Meat science 74.2 (2006): 396-403.
- Estévez, M. "Oxidative damage to poultry: from farm to fork." Poultry science 94.6 (2015): 1368-1378.
- Estévez, M., and C. Luna. "Dietary Protein Oxidation: A Silent Threat to Human Health?." Critical Reviews in Food Science and Nutrition just-accepted (2016): 00-00.
- Esterbauer, Hermann, et al. "The role of lipid peroxidation and antioxidants in oxidative modification of LDL." Free Radical Biology and Medicine 13.4 (1992): 341-390.
- Esterbauer, Hermann. "Cytotoxicity and genotoxicity of lipid-oxidation products." The American journal of clinical nutrition 57.5 (1993): 779S-785S.
- Fang, W., et al. "Effect of oxidated food protein on mice gut floraand redox state." Chinese Journal of Microecology 24 (2012): 193-196.
- Gurer-Orhan, Hande, et al. "Misincorporation of free m-tyrosine into cellular proteins: a potential cytotoxic mechanism for oxidized amino acids." Biochemical Journal 395.2 (2006): 277-284.
- Hou, Jason K., Bincy Abraham, and Hashem El-Serag. "Dietary intake and risk of developing inflammatory bowel disease: a systematic review of the literature." The American journal of gastroenterology 106.4 (2011): 563-573.
- Keshavarzian, A., et al. "Role of reactive oxygen metabolites in experimental colitis." Gut 31.7 (1990): 786-790.
- Keshavarzian, A., et al. "Increases in free radicals and cytoskeletal protein oxidation and nitration in the colon of patients with inflammatory bowel disease." Gut 52.5 (2003): 720-728.
- Li, Zhuqing Leslie, et al. "Effect of oxidized casein on the oxidative damage of blood and digestive organs in mice." Acta Nutrimenta Sinica 35.1 (2013): 39-43.
- Li, Zhuqing Leslie, et al. "Oxidized casein impairs antioxidant defense system and induces hepatic and renal injury in mice." Food and Chemical Toxicology 64 (2014): 86-93.
- Li, Zhuqing Leslie, et al. "24-Week Exposure to Oxidized Tyrosine Induces Hepatic Fibrosis Involving Activation of the MAPK/TGF-β1 Signaling Pathway in Sprague-Dawley Rats Model." Oxidative medicine and cellular longevity 2016 (2015).
- Lund, Marianne N., et al. "Protein oxidation in muscle foods: A review." Molecular nutrition & food research 55.1 (2011): 83-95.
- Sante-Lhoutellier, Veronique, Laurent Aubry, and Philippe Gatellier. "Effect of oxidation on in vitro digestibility of skeletal muscle myofibrillar proteins." Journal of Agricultural and Food Chemistry 55.13 (2007): 5343-5348.
- Siddhuraju, Perumal, and Klaus Becker. "Rapid reversed-phase high performance liquid chromatographic method for the quantification of L-Dopa (L-3, 4-dihydroxyphenylalanine), non-methylated and methylated tetrahydroisoquinoline compounds from Mucuna beans." Food chemistry 72.3 (2001): 389-394.
- Sies, Helmut, Wilhelm Stahl, and Alex Sevanian. "Nutritional, dietary and postprandial oxidative stress." The Journal of nutrition 135.5 (2005): 969-972.
- Soladoye, O. P., et al. "Protein oxidation in processed meat: Mechanisms and potential implications on human health." Comprehensive Reviews in Food Science and Food Safety 14.2 (2015): 106-122.
- Stadtman, Earl R. "Metal ion-catalyzed oxidation of proteins: biochemical mechanism and biological consequences." Free Radical Biology and Medicine 9.4 (1990): 315-325.
- Stadtman, E. R. "Oxidation of free amino acids and amino acid residues in proteins by radiolysis and by metal-catalyzed reactions." Annual review of biochemistry 62.1 (1993): 797-821.
- Szijártó, Andras István, et al. "Elevated vascular level of ortho-tyrosine contributes to the impairment of insulin-induced arterial relaxation." (2014).
- Villaverde, Adriana, and Mario Estévez. "Carbonylation of myofibrillar proteins through the Maillard pathway: Effect of reducing sugars and reaction temperature." Journal of agricultural and food chemistry 61.12 (2013): 3140-3147.
- Wang, Thomas J., et al. "2-Aminoadipic acid is a biomarker for diabetes risk." The Journal of clinical investigation 123.10 (2013): 4309-4317.
- Wu, Peiqun, et al. "Advanced oxidation protein products decrease the expression of calcium transport channels in small intestinal epithelium via the p44/42 MAPK signaling pathway." European journal of cell biology 94.5 (2015): 190-203.
- Xie, F., et al. "Advanced oxidation protein products induce intestine epithelial cell death through a redox-dependent, c-jun N-terminal kinase and poly (ADP-ribose) polymerase-1-mediated pathway." Cell death & disease 5.1 (2014): e1006.






































 + Fat Oxid. During Exercise (10%)")








 for Fat Loss & Exercise Performance")